Accounting for Complexity: Aligning Current Payment Models with the Breadth of Care by Different Specialties
One Pagers | Dec 01, 2014
Joshua Freeman, MD; Stephen Petterson, PhD; and Andrew Bazemore, MD, MPH
Family physicians provide care for a wider range of conditions than do most specialists, introducing a high level of complexity into their practice. Historic assumptions associating complexity with the intensity, skill, and training required to aceommodatea single task fail to capture the complexity of identifying and managing many interacting conditions. Payers and policy makers should recognize this dimension of complexity in care and revisit payment criteria.
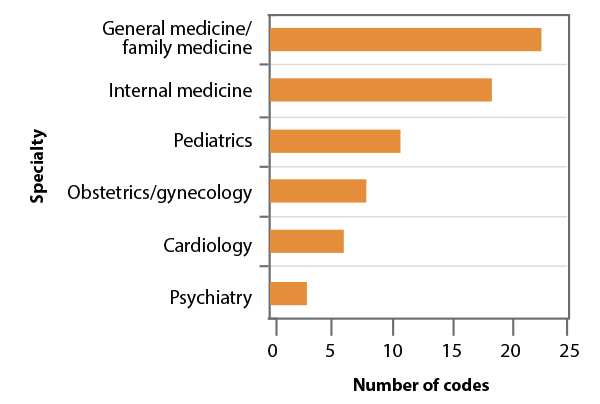
We used data from the 2010 National Ambulatory Medical Care Survey to count how many diagnostic codes were used by primary care physicians and other specialists (see accompanying figure).1 Primary care physicians provide care for a larger number of diagnoses than do specialists. This is exemplified by family physicians, for whom it takes at least 23 diagnostic codes to account for 50% of their coding. In contrast, six diagnostic codes account for 50% of coding for cardiologists, and only three for psychiatrists.1 These findings are consistent with a recent study that calculated the complexity of family physician visits to be 1.3 times that of cardiolo gists and five times that of psychiatrists.2
Figure. Number of diagnostic codes accounting for 50% of coding used by physicians (Information from reference 1)
It has been suggested that the difficulty of professional work may be more associated with how many different tasks are being managed and how they interact witheach other (the complexity of the work) than how difficult any single task is to complete. Even a complicated task, such as managing a single chronic condition, becomes simpler and more routine when it is constantly repeated. Managing a complex adaptive system, such as treatment of a patient with multiple and interactive conditions who is taking multiple drug regimens that may be in conflict, is more complex.4 The more stages there are in the management of each problem and the more problems there are to manage, the higher the skill level needed to perform the task correctly and ensure that what helps one problem does not harm another.5
The Centers for Medicare and Medicaid Services should account for the complexity of the care offered by primary care physicians and the time required to pro vide that care by making adjustments to the fee schedule used to pay physicians.
References
- Centers for Disease Control and Prevention. National Ambulatory Medical Care Survey 2010 http://www.cdc.gov/nchs/ahcd/about_ahcd. htm. Accessed October 1, 2014
- Katerndahl D,Wood R, Jaen CR. Family medicine outpatient encounters are more complex than those of cardiology and psychiatry JAm Board Fam Med. 2011;24(1) 6-15
- Katerndahl D. Providing complex (rather than complicated) chronic care.) J Am Board Fam Med. 2014;27(1) 6-7
- Martin C,Sturmberg J. Complex adaptive chronic care. J Eval Clin Pract. 2009;15(3) 571-577
- Croskerry P, Shapiro M,Campbell S, et al Profiles in patient safety medication errors in the emergency department Acad Emerg Med. 2004;11 (3) 289-299
The information and opinions contained in research from the Graham Center do not necessarily reflect the views or the policy of the AAFP.
Published in American Family Physician, December 1, 2014. Am Fam Physician. 2014::online. This series is coordinated by Sumi Sexton, MD, AFP Associate Medical Editor.