Better Integration of Mental Health Care Improves Depression Screening and Treatment in Primary Care
One Pagers | Nov 01, 2011
Robert L. Phillips, Jr., MD, MSPH; Benjamin F. Miller, PsyD; Stephen M. Petterson, PhD; and Bridget Teevan, MS
Improving screening and treatment for depression in primary care will require better mental health care integration. Depression is common in primary care, yet screening for the condition remains low. Enhanced, coordinated financial support for the integration of mental health care into primary care could improve identification and treatment of depression.
Most people with poor mental health will be diagnosed and treated in the primary care setting.1,2 Depression and anxiety disorders are the most common mental health conditions in primary care, often complicating other medical conditions and making them more expensive.3 Offering treatment for depression after screening can improve outcomes,4 but the U.S. Preventive Services Task Force recommends against screening for depression in primary care unless there are staff-assisted care supports in place to assure accurate diagnosis, effective treatment, and follow-up.5 This is in part a response to evidence that screening alone does not lead to improved outcomes in depression care.4 Staff-assisted supports such as on-site mental health providers and care managers can improve depression identification and treatment. Current health care policy makes it difficult for most primary care practices to integrate mental health staff because of insufficient reimbursement, mental health insurance carve-outs, and difficulty of supporting colocated mental health professionals, to name a few.6
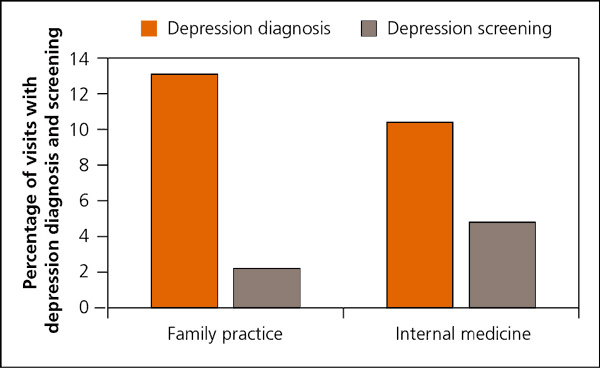
Analysis of National Ambulatory Medical Care Surveys from 2003 to 2006 reveals that despite the high prevalence of depression in primary care (10 to 12 percent), screening is extremely low at 2 to 4 percent (see accompanying figure).7 Primary care physicians can generally tell which patients do not have depression, but often miss those who do.8 Current patterns of screening for depression may be evidence-based given that primary care typically lacks on-site mental health providers, but they are not consistent with making health care more patient-centered, efficient, or effective. Improving identification and treatment of depression in primary care is unlikely to change without better integration of mental health services. Payment and other policies that separate mental health from physical health should be changed to better accommodate care for depression in primary care.
Figure. Percentage of visits with depression diagnosis and screening
References
- deGruy F. Mental health care in the primary care setting. In: Donaldson MS, ed. Primary Care: America's Health in a New Era. Washington, DC: Institute of Medicine; 1996.
- Regier DA, et al. The de facto US mental health and addictive disorders service system. Arch Gen Psychiatry. 1993;50(2):85–94.
- Ani C, et al. Comorbid chronic illness and the diagnosis and treatment of depression in safety net primary care settings. J Am Board Fam Med. 2009;22(2):123–135.
- O'Connor EA, et al. Screening for depression in adult patients in primary care settings. Ann Intern Med. 2009;151(11):793–803.
- USPSTF. Screening for depression in adults. http://www.uspreventiveservicestaskforce.org. Accessed October 4, 2011.
- Kathol RG, et al. Barriers to physical and mental condition integrated service delivery. Psychosom Med. 2010;72(6):511–518.
- Cherry DK, et al. National ambulatory medical care survey: 2006 summary. Adv Data. 2008;(3):1–39.
- Mitchell AJ, et al. Clinical diagnosis of depression in primary care. Lancet. 2009;374(9690):609–619.
The information and opinions contained in research from the Graham Center do not necessarily reflect the views or the policy of the AAFP.
Published in American Family Physician, Nov 1, 2011. Am Fam Physician. 2011;84(9):980. This series is coordinated by Sumi Sexton, MD, AFP Associate Medical Editor.