Greater Family Medicine Presence at NIH Could Improve Research Relevance and Reach
One Pagers | May 15, 2010
Sean C. Lucan, MD, MPH, MS; Andrew W. Bazemore, MD, MPH; Robert L. Phillips JR., MD, MSPH; Imam Xierali, PhD; Stephen Petterson, PhD; and Bridget Teevan, MS
Advisory committees perform pivotal tasks at the National Institutes of Health (NIH), informing funding decisions, helping establish research priorities, and contributing to the vision for the nation's biomedical research agenda. Family medicine has not had a substantial role on these committees, but could, helping the NIH make research more patient centered and informing translational efforts to improve population health.
The NIH, the world's leading biomedical research enterprise, advances new areas of research under the guidance of its advisory committees, which provide peer review, research oversight, and advice on research opportunities. These committees shape how the NIH directs its funding.
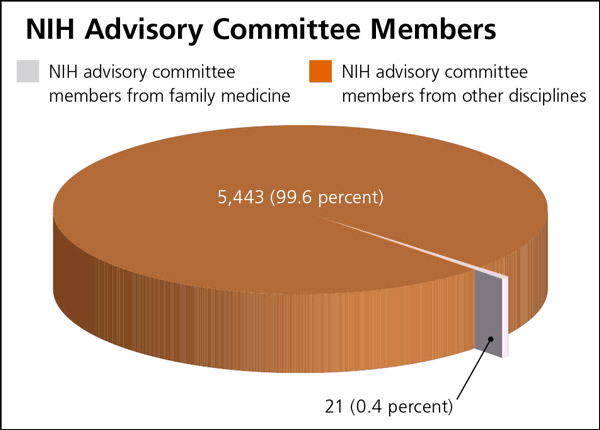
Family medicine has had little role on NIH advisory committees. In 2007, family medicine represented only 21 (0.4 percent) of all 5,464 committee members (see accompanying figure).1 Only 19 (6.4 percent) of the NIH's 295 standing committees had members from departments of family medicine that year.1 Three fourths of NIH institutes and centers had no family medicine input at all.1
Figure. Family medicine versus other disciplines for members of National Institutes of Health (NIH) advisory committees and subcommittees in 2007
Lack of family medicine involvement is a missed opportunity for the NIH. Family medicine—the predominant provider of primary care in the United States2—can offer important insights into real-world patient care. Family medicine practices, where undifferentiated symptoms and conditions first present, are a source of new questions for researchers to explore. Additionally, family medicine conducts a variety of community and practice-based research that can aid in the translation of basic science into clinical practice. Making research more relevant to patient care, proposing clinically relevant research questions, and providing perspective on translation and dissemination are some of the reasons family medicine should participate more on NIH advisory committees.
Although family medicine researchers could join NIH advisory committees as scientific members (i.e., career investigators with established records of research success), family physicians could also serve on committees in public seats (i.e., as nonresearchers having active interest and expertise).3 Public seats must comprise one third of all seats on certain NIH advisory committees by law, and self nomination makes public membership possible.3 More family medicine involvement in scientific and public seats could improve the relevance and reach of NIH research, and thereby improve health for more patients.
References
- Lucan SC, Phillips RL Jr, Bazemore AW. Off the roadmap? Family medicine's grant funding and committee representation at NIH. Ann Fam Med. 2008;6(6):534–542.
- Cherry DK, Woodwell DA, Rechtsteiner EA. National Ambulatory Medical Care Survey: 2005 summary. Adv Data. 2007;(387):1–39.
- NIH. Selection criteria for NIH advisory committees. http://www1.od.nih.gov/cmo/committee/SelectionCriteria2007.pdf. Accessed April 15, 2010.
The information and opinions contained in research from the Graham Center do not necessarily reflect the views or the policy of the AAFP.
Published in American Family Physician, May 15, 2010. Am Fam Physician. 2010;81(10):1213. This series is coordinated by Sumi Sexton, MD, AFP Associate Medical Editor.