Opting Out of Medicaid Expansion May Cost States Additional Primary Care Physicians
One Pagers | Jan 01, 2015
Mark W. Lin, MD; Stephen Petterson, Phd; Claire Gibbons, Phd; Sean Finnegan, MS; Andrew Bazemore, MD, MpH
States currently electing not to expand Medicaid possibly forego the opportunity to expand their primary care workforces by a total of 1,525 physicians. Increased demand from expansion states and a limited primary care physician pool may provide a pull across state lines to the disadvantage of nonexpansion states.
The Affordable Care Act aims to increase health coverage for uninsured Americans, partly through expansion of Medicaid eligibility. To date, 28 states including the District of Columbia have elected to expand this federally funded program, with action pending in two additional states.1 Given that Medicaid expansion has led to increased hiring of primary care physicians (PCPs) in community health centers in expansion states, we aimed to quantify the opportunity cost of not expanding Medicaid by estimating the impact on the primary care workforce in these states.2
Assuming historical patterns of patient encounter per PCP are stable in each state, we estimated the increased demand for PCPs because of Medicaid expansion using a combination of data from the Kaiser Family Foundation, American Community Survey, American Medical Association Masterfile, Medical Expenditure Panel Survey, and the U.S. Census Bureau.3 If the 23 states currently electing not to expand Medicaid had chosen to expand per Affordable Care Act parameters, we estimate the need for 1,525 additional PCPs by 2030. We included states that have not approved Medicaid expansion or have pending waivers for alternative Medicaid plans as of September 2014. By our estimates, the 28 states expanding Medicaid can expect to increase their primary care workforce by 1,312 physicians. The accompanying figure shows the estimated workforce opportunity cost for each nonexpansion state, in proportion to the annual production of primary care providers.3 For example, Texas foregoes the opportunity to expand its primary care workforce by 316 PCPs through 2030. This is equivalent to 67% of its current annual production of 474 PCPs per year.
With evidence of increased hiring of PCPs in Medicaid expansion states, nonexpansion may mean more than a lost opportunity to strengthen a primary care workforce that is already strained by the challenges of caring for an aging and expanding population.4 Increased primary care demand in neighboring expansion states may attract more PCPs away from nonexpanding states. Less access to primary care may lead to worsening access to health care, less access to preventive care, and poorer overall health outcomes. The economic impact of the primary care workforce is also lost in expansion discussions, despite evidence suggesting PCPs generate up to $1.5 million in annual revenues and 23 new jobs apiece.5
Figure. Opportunity costs in states not expanding Medicaid per Affordable Care Act parameters.
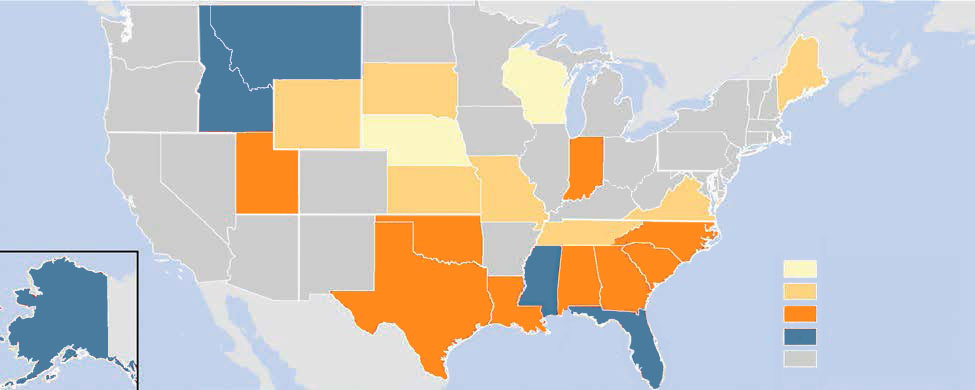 The color codes depict the magnitude of the missed opportunity to expand the primary care workforce through 2030, relative to each state’s annual production of primary care physicians.
The color codes depict the magnitude of the missed opportunity to expand the primary care workforce through 2030, relative to each state’s annual production of primary care physicians.
References
- Kaiser Family Foundation. The cost and coverage implications of the ACA medicaid expansion: national and state-by-state analysis. November 1, 2012. http://kff.org/health-reform/report/the-cost-and-coverage-implications-of-the/. Accessed October 28, 2014.
- Kaiser Family Foundation. Medicaid and community health centers: the relationship between coverage for adults and primary care capacity in medically underserved communities. March 1, 2012. http://kff.org/health-reform/issue-brief/medicaid-and-community-health-centers-the-relationship/. Accessed October 28, 2014.
- Robert Graham Center. Methodology for state-level projections of primary care. Physician workforce. September 1, 2013. http://www.graham-center.org/online/etc/medialib/graham/documents/tools-resources/proj-methology.Par.0001.File.tmp/Methodology_pdf.pdf. Accessed October 28, 2014.
- Petterson SM, Liaw WR, Phillips RL Jr, Rabin DL, Meyers DS, Bazemore AW. Projecting US primary care physician workforce needs: 2010-2025. Ann Fam Med. 2012;10(6):503-509.
- Eilrich FC, Doeksen GA, St. Clair CF. National Center for Rural Health Works. The economic impact of a rural primary care physician and the potential health dollars lost to out-migrating health services. January 2007. http://ruralhealthworks.org/wp-content/files/Physician-Dollars-Jan-2007.pdf. Accessed October 28, 2014.
The information and opinions contained in research from the Graham Center do not necessarily reflect the views or the policy of the AAFP.
Published in American Family Physician, January 1, 2015. Am Fam Physician. 2015;91(1):online. This series is coordinated by Sumi Sexton, MD, AFP Associate Medical Editor.