Rural Origins and Choosing Family Medicine Predict Future Rural Practice
One Pagers | Jun 01, 2007
JL Hyer, MB; Andrew Bazemore, MD, MPH; RC Bowman; Xingyou Zhang, PhD; Stephen Petterson, PhD; Robert Phillips, MD, MSPH
The shortage of physicians in U.S. rural practice may impact access to health care for one in five citizens. Two medical student characteristics that predict eventual practice in rural settings are clear: being born in a rural county and choosing a residency in family medicine.
Although 21 percent of the population of the United States lives in rural areas, only 10 percent of physicians practice there.1 Current trends indicate that rural distribution is declining for all medical specialties, with the nation increasingly dependent on family medicine for rural health care. Family medicine is a key player in the solution for rural health workforce shortages, supplying 58 percent of physicians in isolated rural areas.2
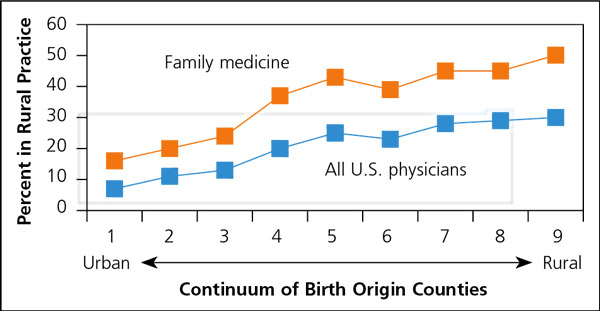
Examination of the birth county of the approximately 540,000 U.S.-born physicians in active, direct patient care shows that students from the most rural counties are four times more likely to practice medicine in a rural area than are those from the most urban counties. The effect of rural origin is even stronger for those entering family medicine3 (see accompanying figure 4,5).
Figure. Impact of birth origin by county on rural practice of the 2006 physician workforce. Information from references 4 and 5.
Barriers to medical training for students of rural origin include lower educational and socioeconomic statuses, fewer role models, less encouragement to pursue higher degrees, fewer academic activities, less technology, and the need to travel to obtain a degree.5 Medical schools may unintentionally create additional hurdles with the trend to higher grade point averages and admission test scores, along with rapidly rising tuition fees.
There are opportunities for medical schools and policy makers to improve disparate access to care in rural areas. Publicly funded medical schools and the legislatures that fund them must consider admissions policies that meet the rural health care needs of their states. This analysis demonstrates that identification of those medical school students most likely to practice in areas of rural health care need is possible. Twenty years of well-documented programs targeting rural-origin students provide examples of tools and policies that effectively increase the number of physicians in rural America.6 Policy makers have the opportunity to create policies that better prepare rural students for health care careers, as well as the authority to require that publicly funded medical schools better meet state physician workforce needs.
References
- Brooks RG, Walsh M, Mardon RE, Lewis M, Clawson A. The roles of nature and nurture in the recruitment and retention of primary care physicians in rural areas: a review of the literature. Acad Med 2002;77:790-8.
- Geyman JP, Hart LG, Norris TE, Coombs JB, Lishner DM. Educating generalist physicians for rural practice: how are we doing? J Rural Health 2000;16:56-80.
- American Medical Association Masterfile, 2006.
- Measuring rurality: rural-urban continuum codes. U.S. Department of Agriculture Economic Research Service, 2006. Accessed March 23, 2007.
- Rourke J, Dewar D, Harris K, Hutten-Czapski P, Johnston M, Klassen D, et al., for the Task Force of the Society of Rural Physicians of Canada. Strategies to increase the enrollment of students of rural origin in medical schools: recommendations from the Society of Rural Physicians of Canada. CMAJ 2005;172:62-5.
- Rabinowitz HK, Diamond JJ, Markham FW, Hazelwood CE. A program to increase the number of family physicians in rural and underserved areas: impact after 22 years. JAMA 1999;281:255-60.
The information and opinions contained in research from the Graham Center do not necessarily reflect the views or the policy of the AAFP.
Published in American Family Physician, Jul 15, 2007. Am Fam Physician. 2007;76(2):207 2. This series is coordinated by Sumi Sexton, MD, AFP Associate Medical Editor.