Family Physicians Contribute Significantly to Emergency Care of Medicare Patients in Urban and Suburban Areas
One Pagers | Sep 15, 2015
Gerald Banks, MD, MS; Peter Wingrove, BS; Stephen Petterson, PhD; and Kathleen Klink, MD
Rural populations rely on physicians trained in primary care to provide emergency services. Less is known about primary care’s contribution to emergency services in urban and suburban settings. Two-thirds of family medicine and three-fourths of general internal medicine Medicare claims for emergency care are generated in urban settings, demonstrating primary care’s significant contribution to the emergency workforce in the most populated areas.
Primary care’s contribution to emergency medicine (EM) in rural areas is well established.1-5 However, this has not been as extensively researched in more urban areas.
A 2007 Institute of Medicine (IOM) report notes that 38% of emergency department (ED) physicians are not board certified in EM, and current rates of EM training may not be adequate for decades, if ever.6 To delineate the current ED service provision, we analyzed 2012 Medicare claims defined by EM Current Procedural Terminology (CPT) codes and sorted them by the U.S. Department of Agriculture’s Rural-Urban Continuum Code (RUCC).7 We cross-referenced these claims with American Medical Association Physician Masterfile data, selected by subspecialty of last completed residency (family, internal, or EM). Of all urban claims, 21% were from family or internal medicine physicians (Figure 1).
Figure. Medicare claims for emergency services (measured by RUCCs).
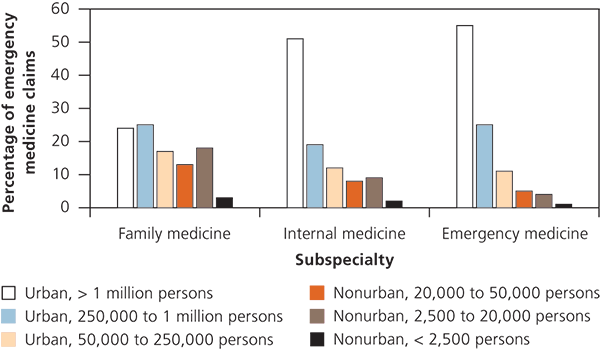
Of the more than 17.3 million 2012 Medicare EM claims, 25% were from primary care physicians (family medicine and general internal medicine). Family physicians provided nearly 12% of the 15 million most urban (RUCC 1 to 3) claims, which is 67% of all family physician claims for the year. This indicates that much of family physician emergency care occurs in non-rural settings. When excluding the most urban areas (RUCC 1) but including other urban areas (RUCC 2 to 3), family physicians’ contribution to emergency care increased to 17% of claims. When categorizing claims by complexity, there was no significant difference between those generated by physicians board certified in EM and those generated by primary care ED physicians in urban areas.
In the setting of lagging EM physician training and increasing ED needs, these findings reinforce the IOM recommendation that credentialing standards should\ emphasize universal core competencies and physician experience rather than only board certification. A shift in the credentialing standards may benefit ED physician recruitment and assure that emergency physicians are qualified, regardless of board certification.
References
- Counselman FL, et al. A study of the workforce in emergency medicine: 2007. Am J Emerg Med. 2009;27(6):691-700.
- Family physicians help meet the emergency care needs of rural America. Am Fam Physician. 2006;73(7):1163.
- Petterson S, et al. One in fifteen family physicians principally provide emergency or urgent care. J Am Board Fam Med. 2014;27(4):447-448.
- Williams JM, et al. Emergency medical care in rural America. Ann Emerg Med. 2001;38(3):323-327.
- Peterson LE, et al. Nonemergency medicine-trained physician coverage in rural emergency departments. J Rural Health. 2008;24(2):183-188.
- Institute of Medicine. Hospital-Based Emergency Care: At the Breaking Point. Washington, DC: National Academies Press; 2007.
- Measuring rurality. USDA. http://www.ers.usda.gov/data-products/rural-urban-continuum-codes.aspx. Accessed February 2015.
The information and opinions do not necessarily reflect AAFP views. Author disclosure: No relevant financial affiliations.
Published in American Family Physician, September 15, 2015. Am Fam Physician. 2015;92(6):445. This series is coordinated by Sumi Sexton, MD, AFP Associate Medical Editor.