Health Care Transition
One Pagers | Dec 01, 2012
Patricia A. Stoeck, Md; Newton Cheng, Ms; Anne J. Berry, Ba; Andrew W. Bazemore, Md, Mph; And Robert L. Phillips, Jr., Md, Msph
Youth with special health care needs who receive care within a patient-centered medical home (PCMH) are significantly more likely to receive services for transitioning to adult care. Broader implementation of the PCMH may contribute to wider use of health care transition counseling and enhanced support for such patients as they prepare to enter adulthood.
With advancements in the treatment of chronic conditions in children over the past 20 years, more than 90 percent of youth with special health care needs will survive into adulthood.1 As such, millions of patients will transition from more family-centered childhood models of care to adult models of care in order to receive more developmentally appropriate care, to facilitate access to adult specialty health care professionals, and to maintain the long-term benefits of primary and preventive care. The need to orchestrate this transition is a Healthy People 2020 objective.2 Best practices for health care transition have been formulated in the context of the PCMH, which aims to provide family-centered, continuous, and comprehensive care.3,4
Figure. Proportion of youth (12 to 17 years of age) with special health care needs in the United States who receive health care transition counseling.
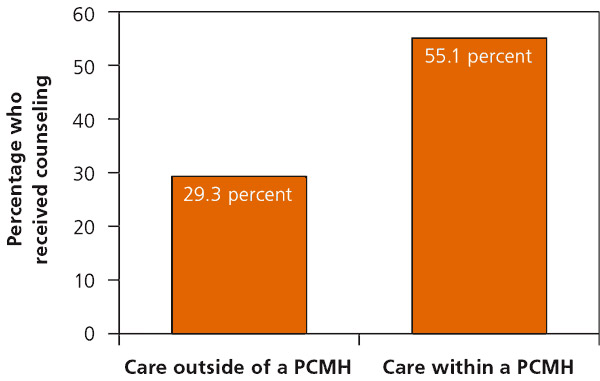 (PCMH = patient-centered medical home) Information from reference 5
(PCMH = patient-centered medical home) Information from reference 5
According to the 2009 to 2010 National Survey for Children with Special Health Care Needs, only 40 percent of youth with special health care needs participate in health care transition counseling.5 Those who obtain care within a PCMH, however, are almost three times more likely to receive transition services than those who receive care outside of a PCMH (odds ratio = 2.96; 95% confidence interval, 2.94 to 2.97; see accompanying figure).5 The association between the PCMH and transition counseling merits further investigation, but may be explained by the inherent ability of the PCMH to facilitate coordinated care and discussions about health care transition. To ensure that all youth with special health care needs successfully transition to adult care, widespread adoption of the PCMH will likely be critical. Training programs that focus on PCMH transformation and legislation for reimbursement of care coordination are key to increasing the number of these youth who receive this valuable care planning.
References
- Blum RW. Transition to adult health care: setting the stage. J Adolesc Health. 1995;17(1):3-5.
- U.S. Department of Health and Human Services. Healthy People 2020 summary of objectives. http://www.healthypeople.gov/2020/topics objectives2020/pdfs/Disability.pdf. Accessed May 25, 2012.
- Cooley WC, Sagerman PJ; American Academy of Pediatrics; American Academy of Family Physicians; American College of Physicians; Transitions Clinical Report Authoring Group. Supporting the health care transition from adolescence to adulthood in the medical home. Pediatrics. 2011;128(1):182-200.
- Medical Home Initiatives for Children with Special Needs Project Advisory Committee; American Academy of Pediatrics. The medical home. Pediatrics. 2002;110(1 pt 1):184-186.
- Data Resource Center for Child and Adolescent Health; Child and Adolescent Health Measurement Initiative (CAHMI). 2009-2010 National survey of children with special health care needs. Indicator data set. http://www.childhealthdata.org/learn. Accessed May 25, 2012
The information and opinions contained in research from the Graham Center do not necessarily reflect the views or the policy of the AAFP.
Published in American Family Physician, Dec 1, 2012. Am Fam Physician. 2012;86(11):235. This series is coordinated by Sumi Sexton, MD, AFP Associate Medical Editor.