Loss of Primary Care Residency Positions Amidst Growth in Other Specialties
One Pagers | Jul 15, 2010
Nicholas A. Weida, BA; Robert L. Phillips, Jr., MD, MSPH; Andrew W. Bazemore, MD, MPH;, Martey S. Dodoo, PhD; Stephen M. Petterson, PhD; Imam Xierali, PhD; and Bridget Teevan, MS
Since the 1997 Balanced Budget Act capped funding for graduate medical education (GME) programs, overall growth in GME has continued (+7.8 percent), but primary care specialties have experienced a substantial decline in their number of programs and residency positions. This decline will further exacerbate the current primary care shortage and severely affect future projections of primary care shortage.
Access to primary care leads to superior health outcomes and decreased costs, yet vast regions of the United States are classified as shortage areas, and 30 percent of the population reports trouble accessing primary care.1,2 Estimates of increased demand from population growth and aging—which preceded health care reform that will insure 32 million more Americans—predict a shortage of at least 35,000 primary care physicians by 2020.3 The physician training pipeline is not prepared to meet this need.
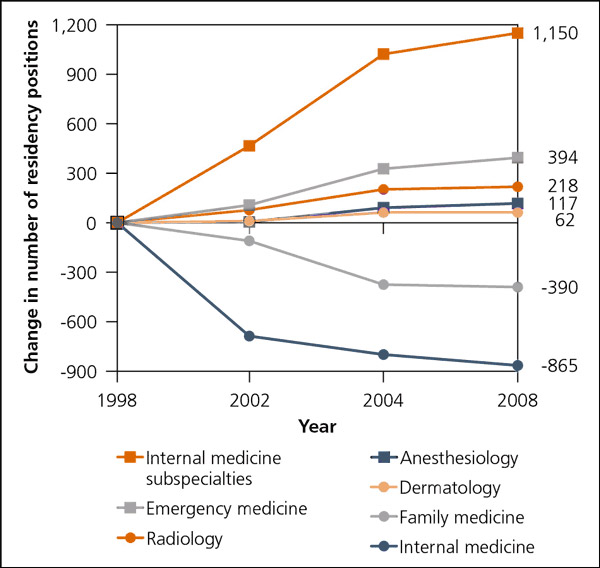
Despite a cap on Medicare funded positions, 9,100 accredited GME positions were created between 1998 and 2008.4–9 Growth was predominantly in subspecialty training and non-primary-care core specialties. Amidst this growth, there was a net loss of 390 first-year family medicine resident positions (see accompanying figure).4,6,7,9 Additionally, 865 general internal medicine positions were lost, converted to preliminary year positions, or offset by opportunities to subspecialize. Primary care also lost 40 family medicine and 25 internal medicine programs during this time.5,7,8,10 Meanwhile, 133 internal medicine subspecialty programs opened.
Figure. Cumulative change in the number of first-year residency positions by specialty available from 1998 to 2008.
There is a mismatch between population workforce needs and residency training changes over the past decade. The Council on Graduate Medical Education recently transmitted concerns about the use of GME to meet hospital financial needs rather than the health care needs of the country.10 Congress and the Centers for Medicare and Medicaid Services should consider ways to increase GME accountability to population needs.
References
- Macinko J, et al. The contribution of primary care systems to health outcomes within Organization for Economic Cooperation and Development (OECD) countries, 1970–1998. Health Serv Res. 2003;38(3):831–865.
- Hackbarth GM. Pursuit of an expanded physician supply. N Engl J Med. 2008;359(7):764.
- Colwill JM, et al. Will generalist physician supply meet demands of an increasing and aging population? Health Aff (Millwood). 2008;27(3):w232–w241.
- Dunn MR, et al. Graduate medical education, 1997–1998. JAMA. 1998;280(9):809–812.
- Graduate medical education. JAMA. 1999;282(9):893–906.
- Graduate medical education. JAMA. 2002;288(9):1151–1164.
- Graduate medical education. JAMA. 2004;292(9):1099–1113.
- Brotherton SE, Etzel SI. Graduate medical education, 2005–2006. JAMA. 2006;296(9):1154–1169.
- Brotherton SE, Etzel SI. Graduate medical education, 2007–2008. JAMA. 2008;300(10):1228–1243.
- Robertson RG, Phillips RL Jr. COGME—May 5, 2009, letter. https://www.hrsa.gov/sites/default/files/hrsa/advisory-committees/graduate-medical-edu/letters/20090505.pdf. Accessed July 5, 2009.
The information and opinions contained in research from the Graham Center do not necessarily reflect the views or the policy of the AAFP.
Published in American Family Physician, Jul 15, 2010. Am Fam Physician. 2010;82(2):121. This series is coordinated by Sumi Sexton, MD, AFP Associate Medical Editor.